As the COVID-19 case count continues to tick upward, the US Food and Drug Administration has approved an updated vaccine for use ahead of the northern hemisphere winter. The emergency use authorization covers updated mRNA vaccines from both Pfizer and Moderna.
The booster shots will target the JN.1 and KP.2 strains of SARS-CoV-2, both of which are omicron variants. Last year’s booster keyed on omicron subvariant XBB.1.5, which has long since lost the evolutionary arms race.
Both Spikevax (Moderna) and Comirnaty (Pfizer) vaccines have been updated. While the vaccine is targeted toward those 12 and over, parents of children aged six months through 11 years are also eligible for the updated vaccines under the FDA’s emergency use authorization.
“Vaccination continues to be the cornerstone of COVID-19 prevention,” said Peter Marks, director of the FDA’s Center for Biologics Evaluation and Research. “These updated vaccines meet the agency’s rigorous, scientific standards for safety, effectiveness, and manufacturing quality. Given waning immunity of the population from previous exposure to the virus and from prior vaccination, we strongly encourage those who are eligible to consider receiving an updated COVID-19 vaccine to provide better protection against currently circulating variants.”
Updated vaccines will hit hospitals and pharmacies soon, as Moderna and Pfizer are ready to ship vaccines. Once injected, the boosters will take a couple of weeks to hit peak protection, and they will offer that level of protection for a few months after the shot. Keep that in mind as you think about timing your booster for maximum efficacy.
Enlarge/ Long covid activists attend the Senate Appropriations Subcommittee on Labor, Health and Human Services, Education, and Related Agencies hearing on the “Fiscal Year 2025 Budget Request for the National Institutes of Health,” in Dirksen building on May 23, 2024.
As a summer wave of COVID-19 infections swells once again, a study published this week in the New England Journal of Medicine offers some positive news about the pandemic disease: Rates of long COVID have declined since the beginning of the health crisis, with rates falling from a high of 10.4 percent before vaccines were available to a low of 3.5 percent for those vaccinated during the omicron era, according to the new analysis.
The study, led by Ziyad Al-Aly, chief of research at the VA Saint Louis Health Care System, used data from a wealth of health records in the Department of Veterans Affairs. The researchers ultimately included data from over 440,000 veterans who contracted COVID-19 sometime between March 1, 2020, and January 31, 2022, as well as over 4.7 million uninfected veterans who acted as controls.
Al-Aly and colleagues divided the population into eight groups. People who were infected during the study period were divided into five groupings by the dates of their first infection and their vaccination status. The first group included those infected in the pre-delta era before vaccines were available (March 1, 2020, to June 18, 2021). Then there were vaccinated and unvaccinated groups who were infected in the delta era (June 19, 2021, to December 18, 2021) and the omicron era (December 19, 2021, and January 31, 2022). The uninfected controls made up the final three of eight groups, with the controls assigned to one of the three eras.
On the decline
In the pre-delta/pre-vaccine era, 10.42 out of 100 unvaccinated people infected developed long COVID in the year after their infection, which the researchers referred to as PASC, or postacute sequelae of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. In the delta era, the rate of long COVID among the unvaccinated fell slightly to 9.51 out of 100. But for the vaccinated, the rate fell much further, to 5.35 out of 100. A similar pattern was seen in the omicron era. For the unvaccinated, the rate of long COVID again fell slightly to 7.76 per 100 people, while the vaccinated saw their rate fall to 3.5 per 100.
In a secondary statistical analysis, called a decomposition analysis, the researchers found that vaccines could explain about 72 percent of the cumulative decline in long COVID rates across the eras, while era-related factors explained about 28 percent. Those era-related factors could include differences in the virus, improved treatments, and use of anti-viral medications.
Further, looking at data on the disease categories related to long COVID cases, the researchers also did an analysis finding a shift in symptoms over the eras. The researchers looked at over 10 disease categories: cardiovascular, coagulation and hematologic, fatigue, gastrointestinal, kidney, mental health, metabolic, musculoskeletal, neurologic, and pulmonary. Compared to the two earlier eras, the researchers noted an increase in gastrointestinal, metabolic, and musculoskeletal diseases involved in long COVID cases in the omicron era.
Overall, the study points to a welcomed decline in the rates of long COVID among the infected, particularly for those who are vaccinated. But, it also makes clear that long COVID isn’t a thing of the past: “a substantial residual risk of PASC remains among vaccinated persons who had SARS-CoV-2 infection during the omicron era,” Al-Aly and his colleagues conclude.
The study also has some limitations, leaving lingering questions for further study. One is whether the type or number of vaccines affect the risk of long COVID—that was not included in the study. The study also didn’t allow researchers to assess whether repeat infections increase the burden of long COVID.
On Wednesday, the Supreme Court tossed out claims that the Biden administration coerced social media platforms into censoring users by removing COVID-19 and election-related content.
Complaints alleging that high-ranking government officials were censoring conservatives had previously convinced a lower court to order an injunction limiting the Biden administration’s contacts with platforms. But now that injunction has been overturned, re-opening lines of communication just ahead of the 2024 elections—when officials will once again be closely monitoring the spread of misinformation online targeted at voters.
In a 6–3 vote, the majority ruled that none of the plaintiffs suing—including five social media users and Republican attorneys general in Louisiana and Missouri—had standing. They had alleged that the government had “pressured the platforms to censor their speech in violation of the First Amendment,” demanding an injunction to stop any future censorship.
Plaintiffs may have succeeded if they were instead seeking damages for past harms. But in her opinion, Justice Amy Coney Barrett wrote that partly because the Biden administration seemingly stopped influencing platforms’ content policies in 2022, none of the plaintiffs could show evidence of a “substantial risk that, in the near future, they will suffer an injury that is traceable” to any government official. Thus, they did not seem to face “a real and immediate threat of repeated injury,” Barrett wrote.
“Without proof of an ongoing pressure campaign, it is entirely speculative that the platforms’ future moderation decisions will be attributable, even in part,” to government officials, Barrett wrote, finding that an injunction would do little to prevent future censorship.
Instead, plaintiffs’ claims “depend on the platforms’ actions,” Barrett emphasized, “yet the plaintiffs do not seek to enjoin the platforms from restricting any posts or accounts.”
“It is a bedrock principle that a federal court cannot redress ‘injury that results from the independent action of some third party not before the court,'” Barrett wrote.
Barrett repeatedly noted “weak” arguments raised by plaintiffs, none of which could directly link their specific content removals with the Biden administration’s pressure campaign urging platforms to remove vaccine or election misinformation.
According to Barrett, the lower court initially granting the injunction “glossed over complexities in the evidence,” including the fact that “platforms began to suppress the plaintiffs’ COVID-19 content” before the government pressure campaign began. That’s an issue, Barrett said, because standing to sue “requires a threshold showing that a particular defendant pressured a particular platform to censor a particular topic before that platform suppressed a particular plaintiff’s speech on that topic.”
“While the record reflects that the Government defendants played a role in at least some of the platforms’ moderation choices, the evidence indicates that the platforms had independent incentives to moderate content and often exercised their own judgment,” Barrett wrote.
Barrett was similarly unconvinced by arguments that plaintiffs risk platforms removing future content based on stricter moderation policies that were previously coerced by officials.
“Without evidence of continued pressure from the defendants, the platforms remain free to enforce, or not to enforce, their policies—even those tainted by initial governmental coercion,” Barrett wrote.
Judge: SCOTUS “shirks duty” to defend free speech
Justices Clarence Thomas and Neil Gorsuch joined Samuel Alito in dissenting, arguing that “this is one of the most important free speech cases to reach this Court in years” and that the Supreme Court had an “obligation” to “tackle the free speech issue that the case presents.”
“The Court, however, shirks that duty and thus permits the successful campaign of coercion in this case to stand as an attractive model for future officials who want to control what the people say, hear, and think,” Alito wrote.
Alito argued that the evidence showed that while “downright dangerous” speech was suppressed, so was “valuable speech.” He agreed with the lower court that “a far-reaching and widespread censorship campaign” had been “conducted by high-ranking federal officials against Americans who expressed certain disfavored views about COVID-19 on social media.”
“For months, high-ranking Government officials placed unrelenting pressure on Facebook to suppress Americans’ free speech,” Alito wrote. “Because the Court unjustifiably refuses to address this serious threat to the First Amendment, I respectfully dissent.”
At least one plaintiff who opposed masking and vaccines, Jill Hines, was “indisputably injured,” Alito wrote, arguing that evidence showed that she was censored more frequently after officials pressured Facebook into changing their policies.
“Top federal officials continuously and persistently hectored Facebook to crack down on what the officials saw as unhelpful social media posts, including not only posts that they thought were false or misleading but also stories that they did not claim to be literally false but nevertheless wanted obscured,” Alito wrote.
While Barrett and the majority found that platforms were more likely responsible for injury, Alito disagreed, writing that with the threat of antitrust probes or Section 230 amendments, Facebook acted like “a subservient entity determined to stay in the good graces of a powerful taskmaster.”
Alito wrote that the majority was “applying a new and heightened standard” by requiring plaintiffs to “untangle Government-caused censorship from censorship that Facebook might have undertaken anyway.” In his view, it was enough that Hines showed that “one predictable effect of the officials’ action was that Facebook would modify its censorship policies in a way that affected her.”
“When the White House pressured Facebook to amend some of the policies related to speech in which Hines engaged, those amendments necessarily impacted some of Facebook’s censorship decisions,” Alito wrote. “Nothing more is needed. What the Court seems to want are a series of ironclad links.”
Enlarge/ Microbiologist Didier Raoult addresses a press conference on COVID-19 at the IHU medical institute in Marseille on April 20, 2022.
A scientific journal published by Elsevier has reportedly posted a stunning 101 expressions of concern on studies connected to Didier Raoult, a disgraced French microbiologist who gained international prominence amid the pandemic by promoting, with little evidence, that the malaria drug hydroxychloroquine could treat COVID-19—a claim that has now been firmly debunked.
According to Retraction Watch, the journal New Microbes and New Infections posted 101 expressions of concern on Raoult’s works recently, including a 2023 study that drew sharp criticism. The study involved giving hydroxychloroquine to tens of thousands of COVID-19 patients after data indicated that it wasn’t effective and the French government rescinded permission for its use against COVID-19. An op-ed in the major French newspaper Le Monde described the study as “the largest ‘wild’ therapeutic trial known to date.”
The expressions of concern also come as Raoult saw his tenth study retracted, Retraction Watch noted.
While Raoult’s unfounded claims about hydroxychloroquine drew initial attention to his COVID-19-related work—with critics quickly noting flaws and weaknesses in his studies—his high-profile claims led critics and sleuths to dive deeper into his extensive publication record. There, they claim they found evidence of long-standing and egregious ethics violations, which were recently laid out in an investigative report by Science Magazine.
Essentially, critics claim Raoult and the institute that he led until 2021, the Hospital Institute of Marseille Mediterranean Infection (IHU), conducted hundreds of studies on humans without appropriate ethical approval or oversight or adequate consent from all participants, the Science investigation found. The IHU work spanned a wide variety of research topics, which involved collecting a variety of biological samples from patients, including vaginal swabs, feces, blood, urine, and breast milk.
However, critics noted 248 IHU studies that reused the same ethical approval code, “09-022,” despite being very different studies that included different kinds of sampling. The critics claim that the studies required separate ethical approvals and additional oversight. They also found that at least 17 studies relied on vulnerable populations, including refugees and people living in homeless shelters, raising serious questions about consent. Some of the studies were also conducted in African countries, where evidence of local ethical approval was either absent or incomplete.
Raoult told the magazine that his research groups had the appropriate ethical approval and said that his critics, whom he described as stalkers and cyber harassers, did not understand how French biomedical laws work.
In Elsevier’s expressions of concern and a linked “Publisher’s Note” from November, the publisher said that the concern was over “the articles’ adherence to Elsevier’s publishing ethics policies and the appropriate conduct of research involving human participants.” Elsevier is still investigating the matter but indicated that the expressions of concern are added “if it is deemed that there is a particular need to alert readers to serious concerns while [the] investigation is ongoing.”
Raoult has had nearly 50 studies likewise flagged over ethical concerns in PLOS journals, Retraction Watch noted. The latest of his studies to be retracted was in the journal Scientific Reports, with the editors there also stating it was due to a lack of ethical oversight. “The paper cites approval from an institutional ethics committee in France, but samples used in this study were also sourced from Algeria, Saudi Arabia, and Niger,” the retraction notice says. “The Authors were not able to provide documentation of approval from ethics committees in these countries or of compliance with local regulations regarding the use of such samples in research.”
Raoult is currently under criminal investigation in France.
Enlarge/ A view of the Centers for Disease Control and Prevention headquarters in Atlanta.
COVID-19 is becoming more like the flu and, as such, no longer requires its own virus-specific health rules, the Centers for Disease Control and Prevention said Friday alongside the release of a unified “respiratory virus guide.”
In a lengthy background document, the agency laid out its rationale for consolidating COVID-19 guidance into general guidance for respiratory viruses—including influenza, RSV, adenoviruses, rhinoviruses, enteroviruses, and others, though specifically not measles. The agency also noted the guidance does not apply to health care settings and outbreak scenarios.
“COVID-19 remains an important public health threat, but it is no longer the emergency that it once was, and its health impacts increasingly resemble those of other respiratory viral illnesses, including influenza and RSV,” the agency wrote.
The most notable change in the new guidance is the previously reported decision to no longer recommend a minimum five-day isolation period for those infected with the pandemic coronavirus, SARS-CoV-2. Instead, the new isolation guidance is based on symptoms, which matches long-standing isolation guidance for other respiratory viruses, including influenza.
“The updated Respiratory Virus Guidance recommends people with respiratory virus symptoms that are not better explained by another cause stay home and away from others until at least 24 hours after both resolution of fever AND overall symptom are getting better,” the document states. “This recommendation addresses the period of greatest infectiousness and highest viral load for most people, which is typically in the first few days of illness and when symptoms, including fever, are worst.”
“Residual risk”
The CDC acknowledged that the eased isolation guidance will create “residual risk of SARS-CoV-2 transmission,” and that most people are no longer infectious only after 8 to 10 days. As such, the agency urged people to follow additional interventions—including masking, testing, distancing, hygiene, and improving air quality—for five additional days after their isolation period.
“Today’s announcement reflects the progress we have made in protecting against severe illness from COVID-19,” CDC Director Dr. Mandy Cohen said in a statement. “However, we still must use the commonsense solutions we know work to protect ourselves and others from serious illness from respiratory viruses—this includes vaccination, treatment, and staying home when we get sick.”
Overall, the agency argued that a shorter isolation period would be inconsequential. Other countries and states that have similarly abandoned fixed isolation times did not see jumps in COVID-19 emergency department visits or hospitalizations, the CDC pointed out. And most people who have COVID-19 don’t know they have it anyway, making COVID-19-specific guidance moot, the agency argued. In a recent CDC survey, less than half of people said they would test for SARS-CoV-2 if they had a cough or cold symptoms, and less than 10 percent said they would go to a pharmacy or health care provider to get tested. Meanwhile, “The overall sensitivity of COVID-19 antigen tests is relatively low and even lower in individuals with only mild symptoms,” the agency said.
The CDC also raised practical concerns for isolation, including a lack of paid sick leave for many, social isolation, and “societal costs.”
The points are likely to land poorly with critics.
“The CDC is again prioritizing short-term business interests over our health by caving to employer pressure on COVID guidelines. This is a pattern we’ve seen throughout the pandemic,” Lara Jirmanus, Clinical Instructor of Medicine at Harvard Medical School, said in a press release last month after the news first broke of the CDC’s planned isolation update. Jirmanus is a member of the People’s CDC, a group that advocates for more aggressive COVID-19 policies, which put out the press release.
Another member of the group, Sam Friedman, a professor of population health at NYU Grossman School of Medicine, also blasted the CDC’s stance last month. The guidance will “make workplaces and public spaces even more unsafe for everyone, particularly for people who are high-risk for COVID complications,” he said.
COVID and flu
But, the CDC argues that the threat of COVID-19 is fading. Hospitalizations, deaths, prevalence of long COVID, and COVID-19 complications in children (MIS-C) are all down. COVID-19 vaccines are safe and effective at preventing severe disease, death, and to some extent, long COVID—we just need more people to get them. Over 95 percent of adults hospitalized with COVID-19 in the 2023–2024 respiratory season had no record of receiving the seasonal booster dose, the agency noted. Only 22 percent of adults got the latest shot, including only 42 percent of people ages 65 and older. In contrast, 48 percent of adults got the latest flu shot, including 73 percent of people ages 65 and older.
But even with the crummy vaccination rates for COVID-19, a mix of past infection and shots have led to a substantial protection in the overall population. The CDC even went as far as arguing that COVID-19 deaths have fallen to a level that is similar to what’s seen with flu.
“Reported deaths involving COVID-19 are several-fold greater than those reported to involve influenza and RSV. However, influenza and likely RSV are often underreported as causes of death,” the CDC said. In the 2022–2023 respiratory virus season, there were nearly 90,000 reported COVID-19 deaths. For flu, there were 9,559 reported deaths, but the CDC estimates the true number to be between 18,000 and 97,000. In the current season, there have been 32,949 reported COVID-19 deaths to date and 5,854 reported flu deaths, but the agency estimates the real flu deaths are between 17,000 and 50,000.
“Total COVID-19 deaths, accounting for underreporting, are likely to be higher than, but of the same order of magnitude as, total influenza deaths,” the agency concluded.
In all, the CDC was ready to fold SARS-CoV-2 into the gang of common seasonal respiratory viruses, with most cases mild and undiagnosed. “Viruses cause most acute respiratory illnesses, but it is rarely possible to determine the type of virus without testing, and oftentimes testing does not change clinical management,” the agency wrote.
Enlarge/ The Moderna Spikevax COVID-19 vaccine is shown at a CVS in 2023.
People ages 65 and up should get another dose of a COVID-19 vaccine this spring, given the age group’s higher risk of severe disease and death from the pandemic virus, the Centers for Disease Control and Prevention announced Wednesday.
Earlier today, an advisory committee for the CDC voted overwhelmingly in favor of recommending the spring booster dose. And late this afternoon, CDC Director Mandy Cohen signed off on the recommendation, allowing boosting to begin.
“Today’s recommendation allows older adults to receive an additional dose of this season’s COVID-19 vaccine to provide added protection,” Cohen said in a statement. “Most COVID-19 deaths and hospitalizations last year were among people 65 years and older. An additional vaccine dose can provide added protection that may have decreased over time for those at highest risk.”
The spring booster will be an additional shot of the 2023–2024 COVID-19 vaccines made by Pfizer-BioNTech, Moderna, and Novavax. The booster dose should be taken after at least four months have passed since a previous COVID-19 vaccination. However, as FDA representative David Kaslow noted in today’s advisory committee meeting, the FDA will likely approve a 2024–2025 version of COVID-19 vaccines for this coming fall. Given that, it’s best for people to get their spring booster dose by the end of June, so they can be ready for another booster before the winter when COVID-19 has generally peaked.
A report published earlier this month by the CDC found that the 2023–2024 COVID-19 vaccine was about 54 percent effective at preventing symptomatic COVID-19 when compared against people who had not received the latest vaccine. However, the CDC estimates that only about 22 percent of adults in the US have gotten a COVID-19 booster this season, and just over 40 percent of people ages 65 and up have gotten the shot.
People over age 65 made up 67 percent of COVID-19 hospitalizations between October 2023 and January 2024, according to CDC data presented at today’s advisory committee meeting. In early January, COVID-19 hospitalizations hit a seasonal high of about 35,000 weekly new admissions per week and nearly 2,500 weekly deaths.
The advisers debated how to word their recommendation for a spring booster and whether getting a booster should require consulting with a health care provider. But, ultimately, the committee decided on a more permissive recommendation, allowing anyone in the age group who wants a booster to be able to freely get one, including at convenient locations, such as local pharmacies.
“Data continues to show the importance of vaccination to protect those most at risk for severe outcomes of COVID-19,” the CDC said in its announcement of the recommendation. “An additional dose of the updated COVID-19 vaccine may restore protection that has waned since a fall vaccine dose, providing increased protection to adults ages 65 years and older.”
The CDC noted that its previous recommendations allow people who are immunocompromised to get additional doses of the COVID-19 vaccines.
For some, having to work from home during the COVID-19 pandemic was stressful. Parents balanced job duties while caring for children. Some struggled to set up a home office and adjust to new tools, like video conferencing. Lonely workdays at home added to social isolation. The line between work and life blurred.
For others, working from home was a boon—comfort, convenience, flexibility, no commuting or rush-hour traffic, no office-environment distractions. When the acute aspects of the pandemic receded, some who at first struggled began to settle into a work-from-home (WFH) groove and appreciated the newfound flexibility.
Then, bosses began calling their employees back to the office. Many made the argument that the return-to-office (RTO) policies and mandates were better for their companies; workers are more productive at the office, and face-to-face interactions promote collaboration, many suggested. But there’s little data to support that argument. Pandemic-era productivity is tricky to interpret, given that the crisis disrupted every aspect of life. Research from before the pandemic generally suggested remote work improves worker performance—though it often included workers who volunteered to WFH, potentially biasing the finding.
For a clearer look at the effect of RTO policies after the pandemic, two business researchers at the University of Pittsburgh examined a sample of firms on the S&P 500 list—137 of which had RTO mandates and 320 that clearly did not between June 2019 and January 2023. The researchers collected publicly available data on each company, including financial data and employee reviews. They then looked at what factors were linked to whether a firm implemented an RTO policy—such as the company’s size, financial constraints, and CEO characteristics—as well as the consequences of the RTO mandates—employee satisfaction and financial metrics of the firms.
Overall, the analysis, released as a pre-print, found that RTO mandates did not improve a firm’s financial metrics, but they did decrease employee satisfaction.
Drilling down, the data indicated that RTO mandates were linked to firms with male CEOs who had greater power in the company. Here, power is measured as the CEO’s total compensation divided by the average total compensation paid to the four highest-paid executives in the firm.
Before the analysis, the researchers hypothesized that RTO mandates may be used to blame employees for poor firm performance. But, companies that have institutional ownership—such as hedge funds or endowments—would not fall for such a “blame game” and would thus would be less likely to implement an RTO mandate. The data supported those hypotheses. Firms with weaker stock performance before employees were able to return to the office were more likely to enforce RTO mandates. However, institutional ownership decreased the probability of RTO mandates.
Although CEOs often justified RTO mandates by arguing it will improve the company’s performance, “Results of our determinant analyses are consistent with managers using RTO mandates to reassert control over employees and blame employees as a scapegoat for bad firm performance,” the researchers concluded.
Unsurprisingly, the researchers also found that RTO mandates were linked to decreases in employee satisfaction. Specifically, after an RTO mandate, employees’ ratings significantly declined on overall job satisfaction, work-life balance, senior management, and corporate culture. But their ratings of factors unrelated to RTO did not change, indicating that the RTO mandate was driving dissatisfaction.
The study has limitations, including a short time frame to look at long-term outcomes of RTO policies and a time frame that overlapped with a labor shortage. Worker responses may be different in a tight labor market. Still, the study adds some data to the ongoing debate—and feuds—over RTO policies.
More than four years after SARS-CoV-2 made its global debut, the US Food and Drug Administration is still working to clear out the bogus and unproven products that flooded the market, claiming to prevent, treat, and cure COVID-19.
The latest example is an alcohol-based sanitizer meant to be smeared inside the nostrils. According to its maker, the rub can protect you from becoming infected with SARS-CoV-2 and other nasty germs, like MRSA, and that protection lasts up to 12 hours after each swabbing. That all sounds great, but according to the FDA, none of it is proven. In a warning letter released Tuesday, the agency determined the sanitizer, called Nozin, is an unapproved new drug and misbranded.
While ethyl alcohol is used in common topical antiseptics, like hand sanitizers, the FDA does not generally consider it safe for inside the nostrils—and the agency is unaware of any high-quality clinical data showing the Nozin is safe, let alone effective. The FDA also noted that, for general over-the-counter topical antiseptics, calling out specific pathogens it can fight off—like SARS-CoV-2 and MRSA—is not allowed under agency rules without further FDA review. Making claims about protection duration is also not allowed.
The FDA’s warning letter is nothing to sneeze at; the letter threatens seizure and injunction for failing to adequately respond.
Nozin’s maker, Maryland-based Global Life Technologies Corp., did not immediately respond to a request for comment from Ars. On its website, the company touts its product’s effectiveness with a link to a published study from 2014, indicating that use of Nozin lowered the colonization levels of S. aureus and other bacteria in the noses of 20 healthy health care workers. The study did not address protection from infection or carriage of any viruses. The company also lists unpublished studies indicating that the product can kill bacteria in laboratory conditions, does not irritate skin, and lowered bacterial growth in the noses of 30 people over a 12-hour period.
To date, the FDA has not approved any nasal sprays to prevent or treat COVID-19, and the scant data on their efficacy remains inconclusive. But there are still plenty of such products for sale online. Most, like Nozin, claim to work by killing bacteria and viruses directly. One product, a nitric oxide nasal spray called Sanotize, is currently in a Phase III clinical trial to test whether it can prevent SARS-CoV-2 infections. Others claim to work by coating the nasal passage with the gelling agent iota-carrageenan to provide a barrier to viral entry. A pilot clinical trial of 400 health care workers in Argentina published in 2021 found that the use of an iota-carrageenan nasal spray led to a 4 percent absolute risk reduction in SARS-CoV-2 infection.
The Centers for Disease Control and Prevention is preparing to update its COVID-19 isolation guidance, moving from a minimum five-day isolation period to one that is solely determined by symptoms, according to a report from The Washington Post.
Currently, CDC isolation guidance states that people who test positive for COVID-19 should stay home for at least five days, at which point people can end their isolation as long as their symptoms are improving and they have been fever-free for 24 hours.
According to three unnamed officials who spoke with the Post, the CDC will update its guidance to remove the five-day minimum, recommending more simply that people can end their isolation any time after being fever-free for 24 hours without the aid of medication, as long as any other remaining symptoms are mild and improving. The change, which is expected to be released in April, would be the first to loosen the guidance since the end of 2021.
In an email to Ars, a CDC spokesperson did not confirm or deny the report, saying only that, “There are no updates to COVID guidelines to announce at this time. We will continue to make decisions based on the best evidence and science to keep communities healthy and safe.”
The Post notes that the proposed update to the guidance matches updated guidance from California and Oregon, as well as other countries.
The officials who spoke with the outlet noted that the loosened guidelines reflect that most people in the US have developed some level of immunity to the pandemic coronavirus from prior infections and vaccinations.
A report earlier this month found that the 2023–2024 COVID-19 vaccine was about 54 percent effective at preventing symptomatic COVID-19 when compared against people who had not received the latest vaccine. However, the CDC estimates that only about 22 percent of adults have received the updated shot.
Currently, the CDC recommends that people wear a mask for 10 days after testing positive unless they have two negative tests 48 hours apart. The Post reported that it’s unclear if the CDC will update its mask recommendation.
Enlarge/ The influenza virus from an image produced from an image taken with transmission electron microscopy. Viral diameter ranges from around 80 to 120 nm.
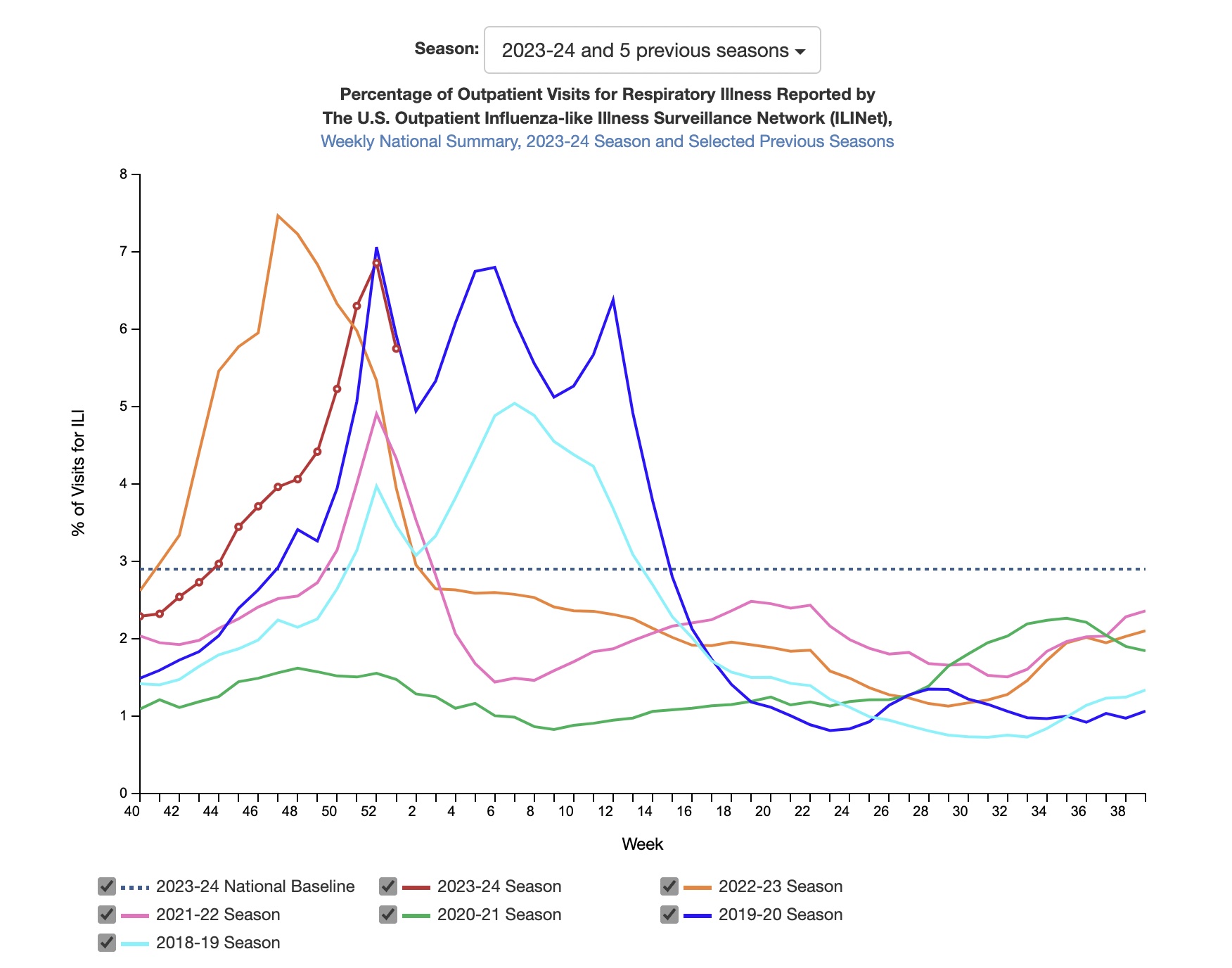
Key indicators of seasonal flu activity declined in the first week of the year, signaling a possible reprieve from the high levels of respiratory virus transmission this season—but the dip may only be temporary.
On Friday, the Centers for Disease Control and Prevention released its latest flu data for the week ending on January 6. Outpatient visits for influenza-like illnesses (ILI) were down that week, the first decline after weeks of rapid increases. Flu test positivity and hospitalizations were also down slightly.
Enlarge/ Percent of outpatient visits for respiratory illnesses by week.
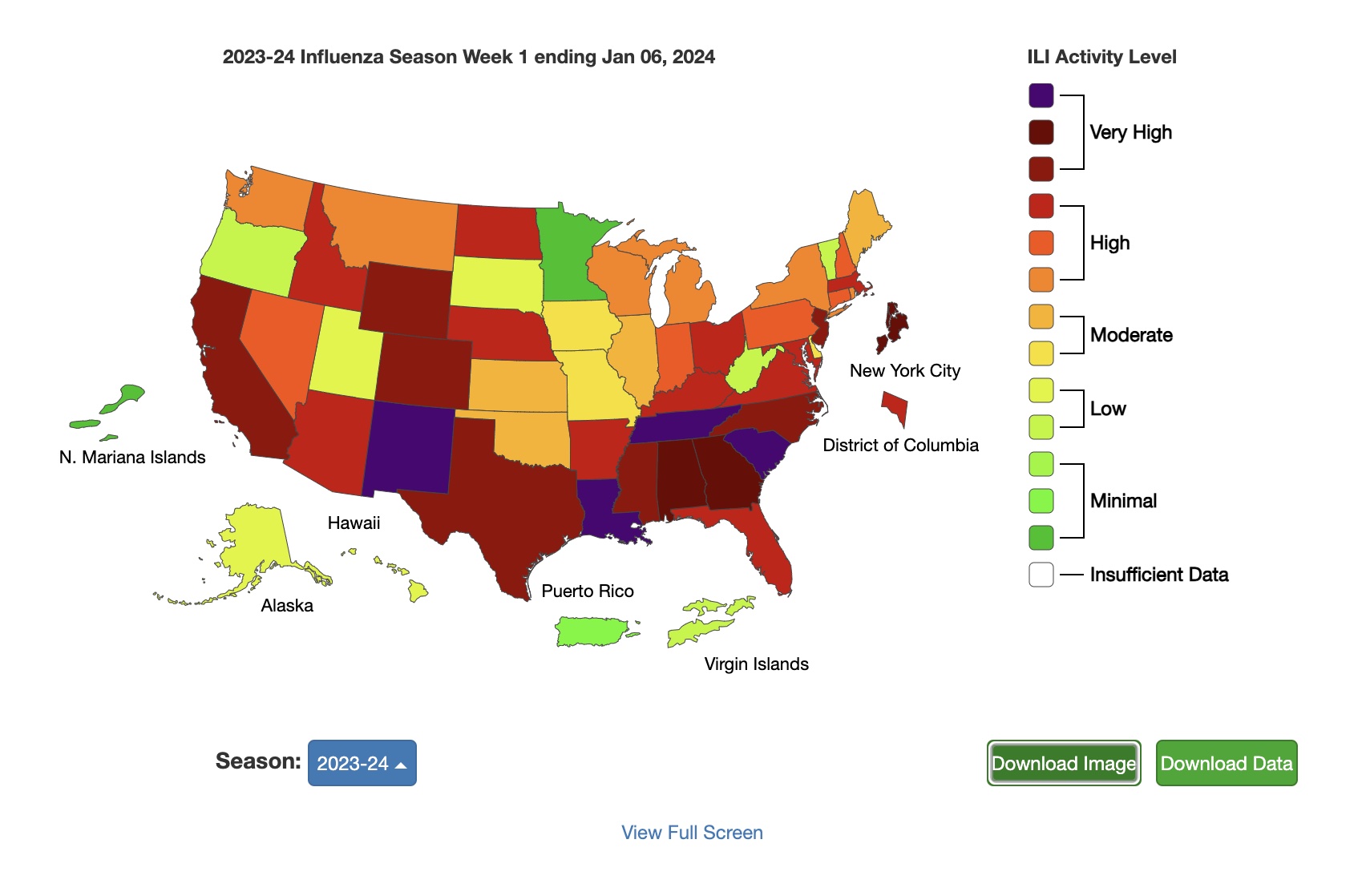
But transmission is still elevated around the country. Fourteen states have ILI activity at the “very high” level in the current data, down from 22 the week before. And 23 states have “high” activity level, up from 19 the week before. (You can see the week-by-week progression of this year’s flu season in the US here.)
The CDC says it is monitoring for “a second period of increased influenza activity that often occurs after the winter holidays.”
Flu isn’t the only virus that seems to be letting up a little in the data, at least for now. COVID-19 data also showed some dips, with the CDC reporting that “Despite test positivity (percentage of tests conducted that were positive), emergency department visits, and hospitalizations remaining elevated nationally, the rates have stabilized, or in some instances decreased, after multiple weeks of continual increase.”
The CDC speculates that some of the declines in indicators could be due to people not seeking medical care during the holidays as they would otherwise. COVID-19 wastewater activity levels remain “very high,” with all regions showing high or increasing levels. The South and Midwest have the highest levels in the latest data, but there are some early indications that rises in the Midwest and Northeast may be slowing down.
Meanwhile, RSV activity remains elevated, though some areas are starting to see declines.
The CDC notes that it’s not too late to get vaccinated against COVID-19, flu, and (for those ages 60 and over) RSV. So far, 21 percent of adults have received the 2023–2024 COVID-19 vaccine, including 41.5 percent of people ages 65 and up. Around 363,000 people have died from COVID-19 in the US since September.
For flu, about 47 percent of adults have received their annual shot, including 74 percent of people ages 65 and up. On Thursday, researchers in Canada published the first estimates of flu vaccine effectiveness this season, finding the current annual shots are 61 percent effective against the most common strain of flu circulating in the US (influenza A(H1N1)pdm09) and 49 percent effective against the less common influenza A(H3N2) and 75 percent effective against influenza B.
The CDC estimates that there have been at least 14 million flu cases, 150,000 hospitalizations, and 9,400 deaths from flu so far this season so far, the agency reported. In the first week of this year, 13 children died of flu, bringing this season’s total to 40.
Enlarge/ A vial of the updated 2023-2024 formula of Pfizer’s COVID-19 vaccine at a CVS Pharmacy in Eagle Rock, California, on September 14, 2023.
Staying up to date on COVID-19 vaccines can cut the risk of COVID-related strokes, blood clots, and heart attacks by around 50 percent in people ages 65 years or older and in those with a condition that makes them more vulnerable to those events, according to a new study from the Centers for Disease Control and Prevention.
The finding, published this week in the CDC’s Morbidity and Mortality Weekly Report, should help ease concerns that the shots may conversely increase the risk of those events—collectively called thromboembolic events. In January 2023, the CDC and the Food and Drug Administration jointly reported a preliminary safety signal from their vaccine-monitoring systems that indicated mRNA COVID-19 vaccines may increase the risk of strokes in the 21 days after vaccination of people ages 65 and older. Since that initial report, that signal decreased, becoming statistically insignificant. Other vaccine monitoring systems, including international systems, have not picked up such a signal. Further studies (summarized here) have not produced clear or consistent data pointing to a link to strokes.
In May, the FDA concluded that the evidence does not support any safety concern and reported that “scientists believe factors other than vaccination might have contributed to the initial finding.”
But, the statistical blip could potentially cause lingering concerns. While clinicians had noted lower rates of thromboembolic events among vaccinated people, the authors of the new study noted that, until now, there were no rigorous estimates of how effective COVID-19 vaccines are at preventing those events.
For their analysis, they primarily looked at two groups of patients: A group of 12.7 million Medicare beneficiaries ages 65 and older and a group of around 78,600 Medicare beneficiaries ages 18 and older with end-stage renal disease (ESRD) on dialysis, a condition that increases their risk for thromboembolic events, including COVID-19-related thromboembolic events. Using medical claims records from September 2022 to March 2023, the researchers compared rates of thromboembolic events among the people in those groups that had gotten a bivalent COVID-19 booster dose and those who had only gotten the original monovalent COVID-19 vaccine in the past. To be considered a COVID-related thromboembolic event, the event had to occur within a week of or a month after a COVID-19 diagnosis.
Protective effect
In the group of 12.7 million patients ages 65 and older, about 5.7 million (45 percent) had gotten the bivalent booster, making them up to date on their COVID-19 vaccinations at the time. The remaining 7 million (55 percent) had only gotten the original vaccine.
During the study period, 17,746 patients who were not up to date on their COVID shots got COVID-19 and experienced a COVID-related thromboembolic event. Of the bivalent boosted patients, there were 4,255 COVID-related thromboembolic events. The researchers adjusted for confounding factors, such as age, race, and time of vaccination, and estimated that the bivalent booster was overall 47 percent effective at preventing COVID-related thromboembolic events, which again include strokes, blood clots, and heart attacks.
A sub-analysis including the time since vaccination indicated that the estimated effectiveness waned about two months after receipt of the vaccine, dropping early effectiveness of 54 percent down to 42 percent at 60 days or more.
Among the 78,600 patients ages 18 and up with ESRD, 23,229 (29.5 percent) received a bivalent dose and thus were up to date on their COVID-19 vaccines. The remaining patients (70.5 percent) had only received an original vaccine, and of those, 917 experienced a COVID-19-related thromboembolic event after getting the pandemic virus. Among the up-to-date patients, there were only 123 events. After adjustments, the researchers estimated that the vaccines’ effectiveness against thromboembolic events was 51 percent in this group, which also waned slightly over time.
The study has limitations, such as that it can’t account for previous COVID-19 infections, which could alter people’s risk of developing complications from COVID-19, including thromboembolic events. It relied on medical claims, which have limitations, and it’s possible there are other confounding factors, such as the use of Paxlovid and behavioral differences. Last, Medicare beneficiaries are not representative of the whole population.
But, given the data available, the study authors concluded that it appears the bivalent vaccine dose “helped provide protection against COVID-19–related thromboembolic events compared with more distant receipt of original monovalent doses alone.” The authors recommend that, “to prevent COVID-19–related complications, including thromboembolic events, adults should stay up to date with recommended COVID-19 vaccination.”
It’s summer 2021. You rent a house in the countryside with a bunch of friends for someone’s birthday. The weather’s gorgeous that weekend, so mostly you’re all outside—pool, firepit, hammock, etc.—but you do all sleep in the same house. And then on Tuesday, you get an alert on your phone that you’ve been exposed to SARS-CoV-2, the virus that causes COVID-19. How likely are you to now have it?
To answer that question, a group of statisticians, data scientists, computer scientists, and epidemiologists in the UK analyzed 7 million people who were notified that they were exposed to COVID-19 by the NHS COVID-19 app in England and Wales between April 2021 and February 2022. They wanted to know if—and how—these app notifications correlated to actual disease transmission. Analyses like this can help ensure that an app designed for the next pathogen could retain efficacy while minimizing social and economic burdens. And it can tell us more about the dynamics of SARS-CoV-2 transmission.
Over 20 million quarantine requests
The NHS COVID-19 app was active on 13 to 18 million smartphones per day in 2021. It used Bluetooth signals to estimate the proximity between those smartphones while maintaining privacy and then alerted people who spent 15 minutes or more at a distance of 2 meters or less from a confirmed case. This led to over 20 million such alerts, each of which came with a request to quarantine—quite a burden.
The researchers found that the app did, in fact, accurately translate the duration and proximity of a COVID-19 exposure to a relevant epidemiological risk score. The app assessed a contact’s risk by multiplying the length of contact, the proximity of contact, and the infectiousness of the index case as determined by how long it had been since the index case started showing symptoms or tested positive.
There was an increasing probability of reported infection as the app’s risk score increased: more contacts whom the app deemed were at a high transmission risk did go on to test positive for COVID-19 within the following two weeks than those who were notified but had lower risk levels. (That’s positive tests that were reported by using the app. Some of the high-risk people probably did not test at all, did not report their test results, or did not report them within the allotted time. So this is an underestimation of the correlation between notification of risk and infection.)
More exposure = higher risk
When the researchers separated the factors contributing to the risk of an exposure, they found that duration was the most important indicator. Household exposures accounted for 6 percent of all contacts but 41 percent of transmissions.
One caveat: The app didn’t record any contextual variables that are known to impact transmission risk, like if people live in an urban or rural area, was the meeting indoors or outdoors, was it during the week or over the weekend, was anyone vaccinated, etc. Including such data could make risk assessment more accurate.
Based on their work, the researchers suggest that an “Amber Alert” stage could have been introduced to the app, in which people deemed to have an interim degree of risk would be guided to get a PCR test rather than immediately jumping to quarantine. Including this intermediate Amber Alert population could have significantly reduced the socioeconomic costs of contact tracing while retaining its epidemiological impact or could have increased its effectiveness for a similar cost. Performing analyses like this early on in the next pandemic to determine how it is transmitted might minimize illness and strain on society.














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}