Public health emergency declared amid LA’s devastating wildfires
The US health department on Friday declared a public health emergency for California in response to devastating wildfires in the Los Angeles area that have so far killed 10 people and destroyed more than 10,000 structures.
As of Friday morning, 153,000 residents are under evacuation orders, and an additional 166,800 are under evacuation warnings, according to local reports.
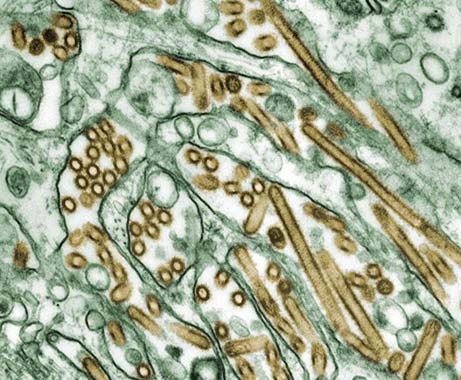
Wildfires pose numerous health risks, including exposure to extreme heat, burns, harmful air pollution, and emotional distress.
“We will do all we can to assist California officials with responding to the health impacts of the devastating wildfires going on in Los Angeles County,” US Department of Health and Human Services (HHS) Secretary Xavier Becerra said in a statement. “We are working closely with state and local health authorities, as well as our partners across the federal government, and stand ready to provide public health and medical support.”
The Administration for Strategic Preparedness and Response (ASPR), an agency within HHS, is monitoring hospitals and shelters in the LA area and is prepared to deploy responders, medical equipment, and supplies upon the state’s request.
Public health emergency declared amid LA’s devastating wildfires Read More »